ABDM Compliance for AB-PMJAY Hospitals
What You Need to Do Before the 2026 Deadline
The National Health Authority has issued a non-negotiable mandate: all 36,229 AB-PMJAY empanelled hospitals must achieve full ABDM compliance before the 2026 deadline — or face suspension, penalties, and de-empanelment.
36,229
Empanelled Hospitals
770M
ABHA Holders
530M
Health Records Digitized
Who This Affects: The Full Scale of the Mandate
This is not a voluntary programme. The NHA has tied AB-PMJAY empanelment directly to ABDM compliance. If you are one of the 36,229 hospitals empanelled under the scheme — public or private — you are required to comply.
19,483
Public hospitals
16,746
Private hospitals
55 crore
Beneficiaries covered
₹1,600 Cr
Allocated over 5 years
What ABDM Compliance Actually Means — In Plain Language
ABDM compliance is structured around three milestones. Each builds on the previous. All three must be completed before go-live.
Patient Identity — The ABHA Layer
- Your HMS/HIS must be able to create ABHA IDs for patients
- Verify existing ABHA IDs at registration
- Link inpatient admissions, outpatient visits, and wellness records to ABHA
- M1 is the foundation — without it, M2 and M3 cannot function
Sharing Health Records — The HIP Role
- Your hospital becomes a Health Information Provider
- Clinical records must be converted to FHIR R4 format
- Each record becomes a "care context" linked to the patient's ABHA
- Patients must consent before any record is shared
- This is the most technically complex milestone
Accessing Patient History — The HIU Role
- Your hospital can now request patient records from other providers
- Doctors can view a patient's complete medical history
- Data is fetched in real time from the Health Information Exchange
- Patient consent is mandatory before access
Beyond the Milestones: Certification and Security — ABDM also requires hospitals to undergo a Web Application Security Assessment (WASA) and receive Safe-to-Host certification from NIC before production credentials are issued by NHA. These security requirements apply regardless of which integration path you choose.
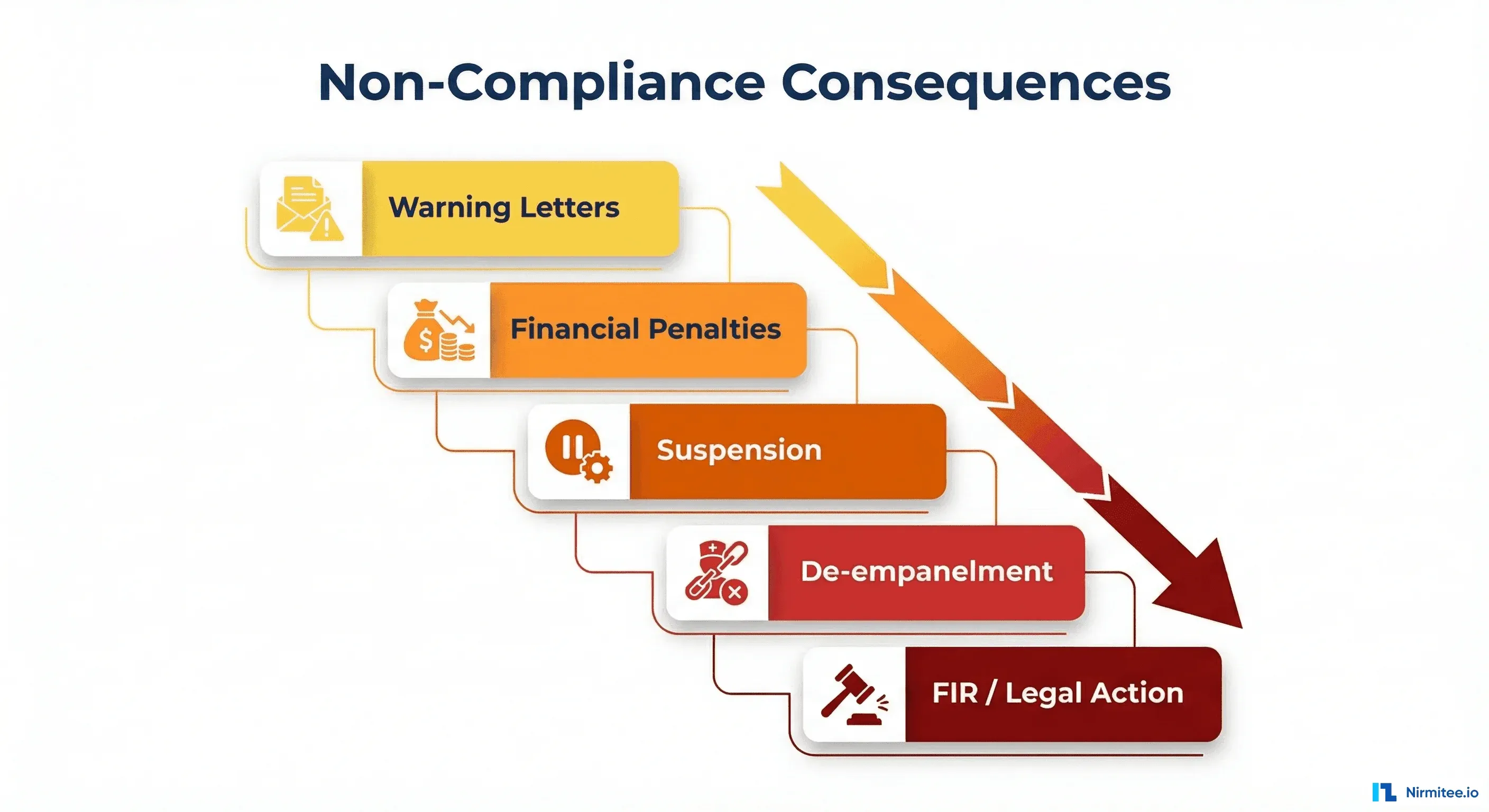
The Consequences of Non-Compliance
The NHA has made clear that non-compliance is not tolerated. The enforcement escalation follows a documented path — and the revenue risk for AB-PMJAY hospitals is existential.
Warning Letters
Documented deadline notices from NHA
Financial Penalties
Monetary fines for continued non-compliance
Suspension
Temporary removal from AB-PMJAY network
De-empanelment
Permanent removal from scheme
FIRs & Legal Action
First Information Reports filed under applicable law
The ABDM Compliance Roadmap: Step by Step
Six concrete steps from assessment to production go-live, each building on the last.
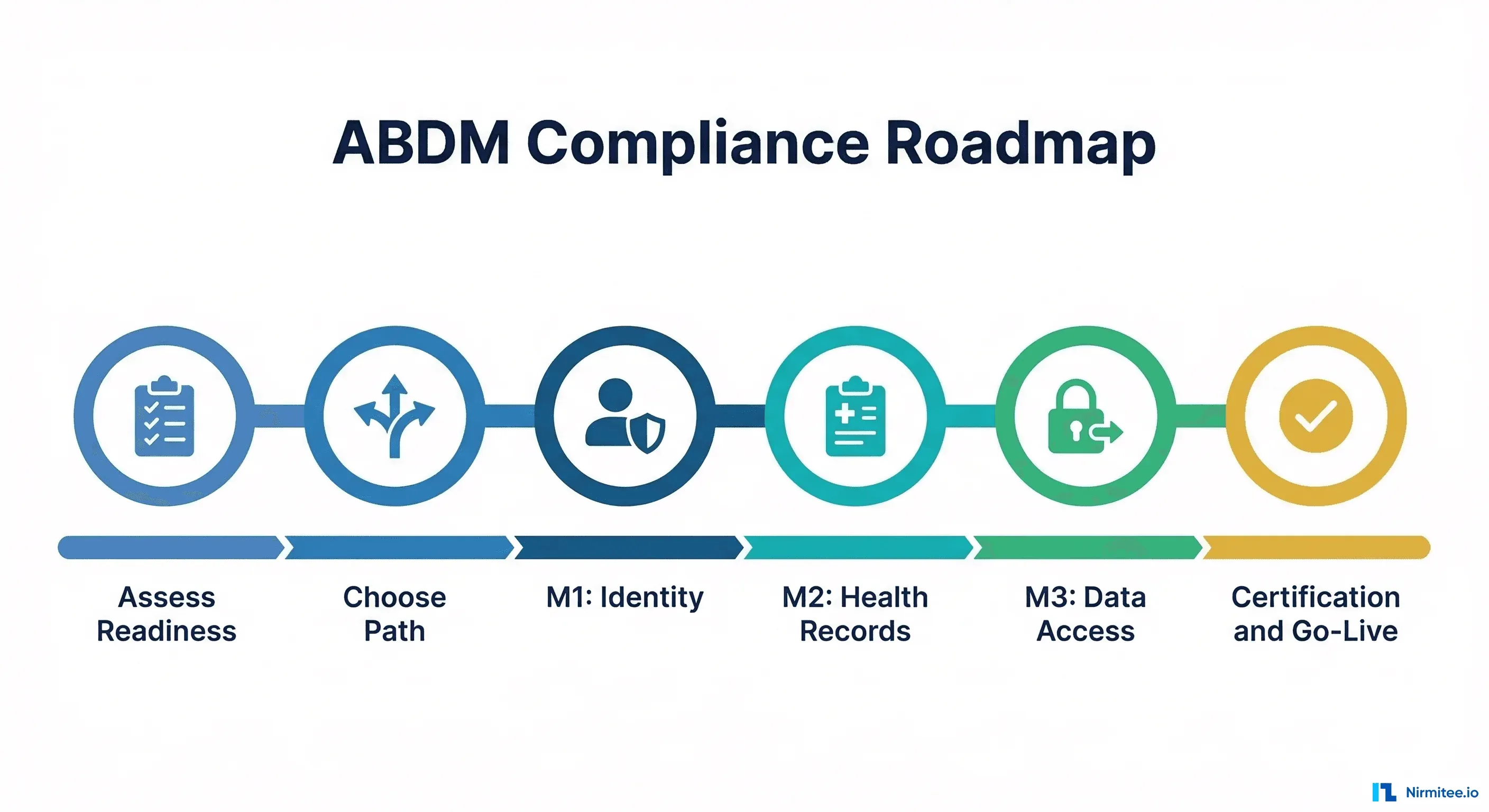
Step 1
Assess Your Current Digital Readiness
Conduct a structured gap analysis of your existing HMS/HIS. Identify whether you have a digital registration system, existing FHIR capability, API connectivity, and security posture. This assessment drives all subsequent decisions.
Step 2
Choose Your Integration Path
Decide between building in-house, buying from a certified vendor, or adding a middleware layer over your existing systems. This decision is irreversible in the short term — get it right.
Step 3
Complete M1 (ABHA Integration)
Integrate ABHA creation and verification into your patient registration workflow. Every admission and visit must be linked to an ABHA ID. This is your compliance foundation.
Step 4
Complete M2 (Health Information Provider)
Implement FHIR R4 conversion for all clinical records. Build care context linkage, consent handling, and the HIE-CM integration layer. This is the most technically demanding milestone.
Step 5
Complete M3 (Health Information User)
Enable your clinicians to request and receive patient records from other ABDM-linked providers. Implement consent request flows and integrate the received data into your clinical workflow.
Step 6
Certification and Go-Live
Complete functional testing with an NHA-empanelled testing agency. Undergo WASA and Safe-to-Host certification. Submit for NHA approval to receive production credentials.
Timeline: How Long You Actually Have
Total estimated duration: 3–8 months from assessment to production go-live. Start now.
| Phase | Duration | Key Activities |
|---|---|---|
| Readiness Assessment | 1–2 weeks | System audit, gap identification, path selection |
| Vendor / Partner Selection | 2–4 weeks | Evaluation, negotiation, contracting |
| M1 Implementation | 2–4 weeks | ABHA creation and verification |
| M2 Implementation | 4–12 weeks | FHIR conversion, care contexts, consent handling |
| M3 Implementation | 2–4 weeks | HIU role, consent requests, data aggregation |
| Functional Testing | 2–4 weeks | NHA-empanelled agency testing |
| WASA + Safe-to-Host | 2–4 weeks | Security audit and infrastructure certification |
| NHA Approval | 2–4 weeks | Review and production credential issuance |
What Small and Mid-Size Hospitals Should Do Differently
Smaller hospitals face unique hurdles that large corporate chains do not. Here's how to address each one.
Outdated or Partially Digital Systems
Many smaller hospitals use standalone billing software or paper-based clinical records. The solution is to adopt a certified middleware layer that bridges your existing setup to ABDM without requiring a full HMS replacement.
Limited IT Staff and Expertise
You don't need an in-house ABDM team. Engage a certified implementation partner who has done multiple go-lives. Define a clear SLA for their support during and after implementation.
Staff Awareness and Training
ABDM compliance is not just a backend IT change. Front-desk staff must learn ABHA ID workflows. Nurses and ward staff must understand care context linking. Build a training programme before go-live.
Consent Management Is Operationally Complex
Patient consent for sharing records must be obtained, recorded, and revocable. Build this into your registration and discharge workflows — it cannot be an afterthought.
Infrastructure Limitations
ABDM integration requires reliable internet connectivity and server uptime for API calls. Assess your current infrastructure against the NHA's technical requirements and budget for upgrades.
Common Mistakes Hospitals Make on the ABDM Journey
Seven implementation pitfalls that delay compliance — and how to avoid each one.
Treating ABDM as a Pure IT Project
ABDM compliance requires changes to clinical workflows, patient registration, consent handling, and staff training. Limiting it to the IT department guarantees operational gaps at go-live.
Starting with M2 Before Getting M1 Right
M1 (ABHA integration) is the foundation. If ABHA creation and linking is inconsistent at registration, every care context created in M2 will have data quality issues that cascade downstream.
Underestimating FHIR Conversion Complexity
Converting existing clinical data to FHIR R4 is not a mapping exercise — it requires understanding of FHIR profiles, resource types, and the specific NHA-mandated implementation guides.
Ignoring the V3 API Migration
NHA deprecated older ABDM APIs and mandated migration to V3. Hospitals or vendors still using deprecated APIs will fail certification. Confirm your vendor's V3 compliance explicitly.
Delaying the Security Audit
WASA and Safe-to-Host certification take 2–4 weeks and require advance scheduling. Hospitals that start the security audit process late miss production go-live windows they cannot recover.
Not Planning for Multi-Software Integration
Most hospitals use different software for billing, lab, pharmacy, and radiology. Each of these systems must be ABDM-connected to produce complete care contexts. Map all your software before implementation.
Waiting for a "Final" Deadline
The NHA has issued and enforced interim deadlines alongside the main mandate. Hospitals that waited for a single final date have already received warning letters. Start now.
We Help Hospitals Achieve ABDM Compliance & AI Automation
AlgoFlow AI specialises in enabling hospitals as ABDM-compliant providers — from custom software builds to plug-and-play integrations. Pick the path that fits your budget and existing infrastructure.
Custom Build
Custom Hospital Software
We design and build a fully custom HMS / clinical module tailored to your hospital workflows, with ABDM M1, M2, M3 compliance built in from day one. Includes FHIR conversion, ABHA integration, consent management, and NHA certification support.
- Full M1, M2, M3 milestone coverage
- Custom workflows for your hospital
- FHIR R4 record conversion included
- WASA & NHA certification support
- AI automation modules available
API Integration
Integrate ABDM into Your Existing Software
Already have an HMS or HIS? We add ABDM compliance as a middleware layer — connecting your existing software to the ABDM ecosystem without replacing it. Fastest path for hospitals with a functional system in place.
- Works with your existing HMS / HIS
- ABHA creation & verification APIs
- FHIR conversion middleware layer
- Consent & care context management
- Ongoing support & updates included
Plug & Play
Independent Ready-to-Use Software
No existing software? No problem. Our ready-to-deploy, ABDM-compliant hospital management platform is live in days — not months. Plug it in, onboard your staff, and start registering ABHA-linked patients immediately.
- Fully ABDM M1, M2, M3 ready
- Deploy in days, not months
- No IT team required
- Training and onboarding included
- AI-powered patient management
Not sure which plan fits? — we'll assess your hospital's current state and recommend the right path.
The Bottom Line
ABDM compliance for AB-PMJAY hospitals is not optional, not postponable, and not a small undertaking. With 36,229 hospitals required to complete M1, M2, and M3, and a realistic implementation timeline of 3–8 months, the only safe choice is to start your assessment today.
The revenue risk is existential for hospitals that derive a significant portion of income from AB-PMJAY reimbursements. De-empanelment is not a temporary inconvenience — it is a structural disruption to your patient pipeline and cash flow.
Frequently Asked Questions
Key questions about ABDM compliance answered.